 Dr. Rhett Drugge is a native of Darien, Connecticut and a graduate of Harvard University. Graduating with a baccalaureate degree in Intellectual History, he went to Washington DC and wrote senatorial speeches for Connecticut Senator Lowell Weicker. A few years later, he distinguished himself in medical research at Yale University by discovering the receptor for cyclosporin A (the major drug for organ transplant patients). He then matriculated to New York Medical College in Valhalla, New York where he went on to receive his medical degree. While a medical student, he served some of his medical rounds at Stamford Hospital. He completed his medical internship at New York University and then served his Dermatology Residency at the University of Michigan.
Dr. Rhett Drugge is a native of Darien, Connecticut and a graduate of Harvard University. Graduating with a baccalaureate degree in Intellectual History, he went to Washington DC and wrote senatorial speeches for Connecticut Senator Lowell Weicker. A few years later, he distinguished himself in medical research at Yale University by discovering the receptor for cyclosporin A (the major drug for organ transplant patients). He then matriculated to New York Medical College in Valhalla, New York where he went on to receive his medical degree. While a medical student, he served some of his medical rounds at Stamford Hospital. He completed his medical internship at New York University and then served his Dermatology Residency at the University of Michigan.
Board Certified in both Dermatology and Dermatologic Surgery in 1992, Dr. Drugge is a member of the Society for Investigative Dermatology, the American Academy of Dermatology, and the American Society for Mohs Surgery. He is the founder of the Internet Dermatology Society and he is the Chief Editor of the Electronic Textbook of Dermatology. Dr. Drugge has written numerous database information systems for networked medical record keeping, with a special focus on physician to physician communications & dermatology information systems. He also designs and tests imaging solutions for the skin care industry.
In 2008 Dr. Drugge was granted a patent for his unique invention, the Melanoscan system for whole body imaging, which aids in the early detection of skin cancers. He is also active in interviewing prospective undergraduates for Harvard.
Dr. Drugge and his wife Heather live in Darien with their three children.

Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.

Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.

Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.

Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.

Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.

Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Are Botox treatments safe?
Botox injections have been used safely and effectively for over ten years to treat many ophthalmological and neurological disorders. Each year thousands of patients receive Botox treatments for a variety of conditions and it has become a popular treatment for reversing the visible signs of aging. Dynamic wrinkles are caused by contractions of the delicate underlying facial muscles every time you smile, laugh or frown. The more emotion you show, the deeper these wrinkles and lines are likely to be. While you may have earned every one of your worry lines, you don’t have to show them anymore.
What is “Botox”?
Botulinum toxin (Botox) is a protein produced by a bacteria called Clostridium botulinum. The effects that this toxin can have on the body have been known since the turn of the century, but in the 1980’s the beneficial, cosmetic effects of Botox were discovered, and turned to our advantage. Botox has a relaxing effect on muscle tissue, thus when it is injected into specific target areas of certain muscle groups those muscles lose some or all of their ability to contract.
How can Botox help me?
Take a look in the mirror and frown at yourself. See where the vertical furrows develop between your brows? Now relax. Can you still see remains of those furrows? Now squint at yourself. See the crows feet develop around your outer eyes? Again, relax. Can you still see where those lines were? If you answered yes to either of those questions then Botox may be helpful to you. The permanent presence of frown lines or crows feet may be due to the over-activity of certain muscle groups. Over time this causes deep wrinkles or furrows to appear, which may result in a prematurely old appearance, or a less than pleasant expression. The injection of Botox into those muscle groups on the forehead and/or around the eyes can help eliminate those furrows, giving a more youthful appearance or a more pleasing demeanor.
What will the results be?
A botox injection can take from 1 to 2 weeks to become fully effective but most people notice the effect within 48 hours. During this period a subtle relaxation of the muscle takes place such that you should not even be aware that it has happened – until you notice that the lines are gone! The ability to frown or squint are also reduced. The treatment is not permanent – one of the benefits of botox injections. The effects will slowly wear off – over a time period which can vary from person to person (from 4 to 6 months). Therefore, if you are dissatisfied with the results you can be reassured that it will wear off. Permanent relaxation of the muscle can be achieved after repeated treatments.
Preparation, the Procedure and After-care
There is no preparation that you need to do other than have a consultation with your physician about your suitability for the treatment. The injections themselves are done with the patient in the sitting position, and a very small, fine needle is used to inject a controlled dose of the toxin into specific areas of the target muscles. The procedure takes no more than a few minutes. There is no aftercare required – you may return to work or the rest of your day’s schedule immediately.
What is the price?
The cost per BOTOX® session is $435 USD. Areas that require more than a single injection, such as the area beside the eyes where so-called “crow’s feet” tend to form, can range from $300 to $1000 USD. Larger surface areas such as the forehead can cost as little as $500 and as much as $1400 USD.
Are Restylane treatments safe?
Significant risks with Restylane injections are infrequent, but the potential side effects to the treatment are:
However these side effects listed above usually disappear within two to three days.
Restylane has been proven to be a safe procedure. Since it is non-animal based, it virtually eliminates the possibility of disease transmission or an allergic reaction. Plus Restylane is biocompatible with human hyaluronic acid.
What is “Restylane”?
Impressions of beauty change with time – as do our faces as we age. With RESTYLANE, you can have a natural beauty lift with the body’s own material. RESTYLANE is a crystal-clear, non-animal, biodegradable gel based on a natural substance, called hyaluronic acid. The gel is injected into the skin in tiny amounts with a very fine needle. The result is instantaneous and produces a long-lasting,natural enhancement, gentle and safe to your skin.
Where Can Restylane Be Used?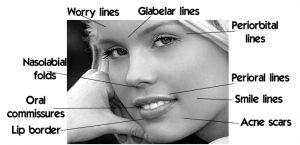
Hyaluronic acid implantation can be used to improve the skin’s contour and reduce depressions in the skin due to scars, injury or lines.
Facial lines and features that can be corrected using these hyaluronic acid fillers are:
How long will the procedure take?
The Restylane injections can take anywhere from a few minutes to an hour, depending on how large of an area needs to be treated.
Another Restylane benefit is that the procedure is completed quickly, so the patient can have it done during a lunch hour. Go to lunch, have the Restylane procedure, and return to work looking younger.
Preparation, the Procedure and After-care
Achieving the look you desire is as easy as it is quick. The result is instantaneous. No previous skin test is needed, which means that you can have the treatment immediately. The session often takes less than thirty minutes. The time differs somewhat depending on the desired correction. During treatment, RESTYLANE is injected into the skin in tiny amounts with a very fine needle. When injected, RESTYLANE produces volume that smoothes the wrinkle or fold, shapes the facial contour or enhances the lips in a natural way. The result is immediate. The method of injecting RESTYLANE is fast, safe and leaves no scars or other traces on the face.
What is the price?
A full Restylane syringe (for e.g., enough to do the lines around the lips) is $500.
Why have a chemical peel?
If your skin is blemished from sun damage, or acne scarring then a chemical peel may be a good remedy for removing the blemishes. Clinical signs of photoaging of the skin include rhytids (wrinkles around the eyes), lentigines (pigmented spots), keratoses, telangiectasia (broken blood vessels), loss of translucency, loss of elasticity, and a sallow color. A consultation with your dermatologist will help determine what kind of peel is best for you, and whether it could be a single treatment or a series of treatments performed over several months.
Chemical peels can effectively improve a wide variety of skin conditions including:
What is a “chemical peel”?
Chemical skin peeling is an established technique for improving or erasing wrinkles, keratoses and areas of increased pigmentation, including freckles, “age or liver spots”, etc. This technique was developed in 1903 by Dr. George Miller McKee – the founder of the practice of Sheard & Drugge.
A chemical peel is the application of an acid to the skin, usually on the face, although any area may be treated. This removes the superficial, damaged layers to reveal new, undamaged skin. The depth of the peel depends on the formulation and the concentration of the acid used. As the procedure has developed, the formulations have greatly improved to allow for a much wider range of desired results – and more comfort and satisfaction for the patient.
What will the immediate results be?
This would depend on the type and strength of the peel done. A mild peel may produce little immediately discernible effects – the effect is more noticeable once the skin layers treated by the acid have sloughed off, usually in a few days. A deeper, more concentrated peel may produce redness that lasts for a couple of weeks, this will gradually fade to reveal the fresh, undamaged skin. A strong, one-step peel can result in what appears to be a second degree burn – intense redness, some blistering. This can last for up to a month or so, until the new layers come up – these strong peels have the worst short-term effects, but produce the best long-term results for badly blemished skin.
Preparation, the Procedure and After-care
Your dermatologist may instruct you to prepare your skin in the week or two prior to the peel by using certain skin products. These preparations help to remove dead skin cells which improves the efficiency of the peel. The peel itself is performed as a normal office visit in which the doctor will clean the skin with alcohol, apply the peel and then, depending on the peel used, either water or a special neutralizing agent. You may experience some mild burning and stinging as the peel works into the skin layers, but this is usually very short lived (a few minutes). After care will depend on the strength of the peel, but is usually very simple and straightforward – however, we don’t recommend the use of makeup for a little while, especially for stronger peels. Therefore you need to be prepared to go around looking a little “rough” for a while if you have a stronger peel performed. Your dermatologist can help you decide if a series of milder peels, or one strong peel is better for your individual needs.
What is the price?
The cost of the chemical peel is $90 USD.
 Acne is driven by sebaceous gland secretions, most common in teenagers, but it can also occur in adults and in the first few weeks of life (transplacental hormone influences) and occasionally starts at age 8 or 9. The face, chest and upper back are the most commonly affected sites although acne may be present on the shoulders, arms, underarms, groin and scalp. Acne may induce lifelong scarring and thereby affect a person’s self-esteem. Acne is as a general rule quite curable, excluding those regions in which scarring has been so severe as to cause cyst formations. Even advanced cases can usually benefit tremendously from dermatologic management, from the simple topical home remedies to the most elaborate scar revisions which may include scar subcision, soft-tissue augmentation and skin resurfacing (the latter involving peels, lasers and abrasive techniques). In some cases, entire face lifting as well as botox may be necessary to control the damage to the patient’s sense of esthetic self-esteem.
Acne is driven by sebaceous gland secretions, most common in teenagers, but it can also occur in adults and in the first few weeks of life (transplacental hormone influences) and occasionally starts at age 8 or 9. The face, chest and upper back are the most commonly affected sites although acne may be present on the shoulders, arms, underarms, groin and scalp. Acne may induce lifelong scarring and thereby affect a person’s self-esteem. Acne is as a general rule quite curable, excluding those regions in which scarring has been so severe as to cause cyst formations. Even advanced cases can usually benefit tremendously from dermatologic management, from the simple topical home remedies to the most elaborate scar revisions which may include scar subcision, soft-tissue augmentation and skin resurfacing (the latter involving peels, lasers and abrasive techniques). In some cases, entire face lifting as well as botox may be necessary to control the damage to the patient’s sense of esthetic self-esteem.
Acne is generally earlier in onset and most severe in young men, where as women suffer from a long, slow acne development process. Biologically speaking, acne is driven by androgenic sex hormones, testosterone and androstenedione. Androgen sensitive hair follicles contain the sebaceous glands which thicken the skin of the face, scalp, ears, neck, upper back, chest shoulders and arms. Ensuing sebaceous secretions overwhelm clogged hair follicle outlets (pores). Acne is not typically caused by infection, but it does set the stage for secondary infections. Sebacous glands reflect nature’s attempts to provide protection from the elements that primitive man encountered. At ages 12-14, boys and girls were expected to make their own way and catch their own food so nature provided them with the hormone of aggression, testosterone. In general, estrogens decrease sebaceous gland activity and androgens increase it. In women, androgens are produced by the ovaries (markedly so in polycystic ovary disease), the placenta and adrenals, and in men by the testes and adrenals. While males experience a peak in testosterone at age 18, female testosterone peaks at 31. Birth control pills by their estrogenic effects have a mild effect on acne. It is occasionally noticed that some of the more androgenic preparations may aggravate acne and even produce mild hirsutism. A certain amount of trial and error for each individual is therefore necessary to pick out the best contraceptive.
Did you know?
Effects of Future Weight Gain
The current belief is that once fat cells have been removed from the body they do not grow back. Future weight gains tend to be distributed more evenly over the body, as weight gain is the result of existing cells swelling. Obviously liposuction removes some of those cells, so weight gain in the treated areas is proportional to the increase in size of remaining cells.
What is Liposuction?
Liposuction was developed in the 1970’s by Georgio Fischer, M.D. of Italy for the removal of fat deposits located in areas that are resistant to diet and exercise, or that are naturally subject to fat deposition. While not a treatment for generalized obesity, this procedure is ideal for the removal of unwanted fat deposits in the face, chin, neck, hips, buttocks, abdomen, knees, calves, chest and breasts.
The Best Candidates for Liposuction
To be a good candidate for liposuction, you must have realistic expectations about what the procedure can do for you. It’s important to understand that liposuction can enhance your appearance and self confidence, but it won’t necessarily change your looks to match your ideal or cause other people to treat you differently. The best candidates for liposuction are normal-weight people with firm, elastic skin who have pockets of excess fat in certain areas. You should be physically healthy, psychologically stable and realistic in your expectations. Your age is not a major consideration; however, older patients may have diminished skin elasticity and may not achieve the same results as a younger patient with tighter skin. Liposuction carries greater risk for individuals with medical problems such as diabetes, significant heart or lung disease, poor blood circulation, or those who have recently had surgery near the area to be contoured.
Preparation, Surgery and Immediately Afterwards
Planning and discussion of liposuction may require one or two consultations before an appointment for the procedure is made. A consent form will be signed by the patient prior to treatment. Prior to having the surgery, patients should refrain from taking any aspirin, (it can interfere with proper blood clotting for at least 10 days).
On the day of the surgery, you may go about your usual routine, eat a light breakfast if the surgery is in the morning or a light lunch if it is in the afternoon. Avoid drinking large quantities of liquid, as the procedure may take 1-3 hours. Be on time for your appointment and wear comfortable loose-fitting clothes. Pre-operative digital photographs will be taken prior to the procedure.
At the surgery, the doctor will mark the areas to be treated and inject local anaesthetic into the areas where he plans to make incisions. Small incisions are then made through which saline and numbing solution will be injected using a blunt-tipped needle. Some discomfort may be felt initially as the solution starts to go in, but that should soon fade as the anaesthetic takes effect. The doctor will inject the solution across the entire area to be treated. (Patients report a feeling more of pressure than discomfort or pain during this). Then, the doctor will insert the instrument (cannula) and start to remove the fat through suction.
You will work with the doctor during the procedure and he will ask you to stand up to assess the smoothness of your new contours (fat lies differently in different positions). If the procedure is on the buttocks, legs or abdomen, we request that you have someone to drive you home and also recommend taking it easy for the first 24 hours, but there is no need to stay completely sedentary. In fact, light activity will help to stimulate healing. Post-operative bruising and discomfort is usually minimal and may be treated with low grade pain-killers such as Tylenol.
A follow up visit two days later is scheduled. You should not expect to be fully able to assess the results for a few months, as the skin recontours to the reduced fat layer. In a month, additional photographs will be taken to compare to the pre-operative photos.
What is the cost of liposuction?
Body site Surgical Fee(US$)
Abdomen, upper & lower $3,000
Arms $2,000
Back $4,000
Breasts, female $2,500
Breasts, male $2,500
Buttocks $2,500
Chin, Cheeks, Jowls, Neck $2,000
Flanks $3,000
Outer Thighs $3,000
Inner Thighs $3,000
Hips/Waist $3,000
Ankles & Knees $2000
Spider veins, or telangiectasias, are those tiny purple and red blood vessels found most commonly on the thigss or lower legs of women. They are hereditary and can form anywhere on the leg, from the top of the thigh to the ankle. Occasionally, spider veins appear on the face.
Varicose veins are larger. They can appear raised, with a bluish color, and can become quite painful. Although spider veins and varicose veins carry blood, they are not part of the venous valve system.
Spider veins are most often treated with sclerotherapy, in which a saline or chemical solution that is injected into the vein, irritating the lining and causing the vein to collapse and disappear.
In some cases, laser treatment may be used either alone or in combination with sclerotherapy.
Did you know?
4. Dr. Drugge was trained in liposuction in his residency and has been performing this safe technique for over ten years.
How is it done?
The softness and suppleness which give the breasts their shape are due mainly to the presence of adipose tissue (fat). Natural Breast Augmentation is an injection technique used to transfer natural adipose tissue from one area of the body to the breasts.
The tissue is alive and as such is treated like a graft. Volumetric measurements of the breasts are taken before each injection series and the adipose tissue is injected in the precise proportion necessary for the greatest survival. The tissue that is retained after three months is considered permanent.
The procedure requires a small extraction (mini-liposuction) procedure from the outer thighs, hips, buttocks, or abdomen. This is done under local anesthesia.
The collected adipose tissue is frozen at -30 C. Some blood is taken for laboratory processing where the platelet enriched plasma is added back to the tissue before injection.
Once the breasts are numb with local anesthesia through a 4mm hole under each breast, the enriched adipose tissue is injected using a blunt cannula into the specific areas of the breasts which need enhancement. The most popular areas for injection are the upper quadrants of the breast which enhance the roundness of the breast and the appearance of cleavage. This technique can also improve breast assymetry.
The breasts are then enlarged gradually over several injection series depending upon the cup size desired. For further information about the procedure, please request a lipsuction pamphlet from Dr. Drugge’s office.
Who is the ideal candidate for NBA?
Small breasts (A cup/B cup) or flat breasts.
Available adipose tissue from another part of the body such as the thighs, hips or abdomen. (Until we develop a way to grow your adipose tissue in vitro, you must have adequate harvest material.)
Pre and Post Procedure Details
Planning and discussion of the harvest and injection procedures may require one or two consultations before an appointment for the procedure is made. Prior to having the surgery, patients should refrain from taking any aspirin, (it can interfere with proper blood clotting for at least 10 days).
Be on time for your appointment and wear comfortable loose-fitting clothes. Pre-operative digital photographs will be taken prior to the procedure.
Bring a sports bra or underwire bra to wear after the procedure. Post-operative discomfort is usually minimal and may be treated with low grade pain-killers such as Tylenol. There may be minimal (1-3 teaspoons) of leakage from the incision holes over the next 24 hours from the anesthesia. This can be pink or yellowish in color.
The patient should not expect to be fully able to assess the results for a few months, as the skin recontours to the enhanced fat layer. In a month, more photographs will be taken to add to the patient’s record and be compared to the pre-operative photos.
Effects of Future Weight Gain or Loss
Since the breasts are sensitive to weight loss, it is not recommended to diet or lose weight. Adipose tissue will shrink with weight loss and swell with weight gain. Some patients have experienced increased breast size on top of the procedure with minimal weight gain.